Free Sample Emergency Medicine Questions, with Answers
See why TrueLearn is a trusted resource for thousands of medical students and residents. At TrueLearn, we understand that it’s all about the content. That’s why we have high-yield emergency medicine practice questions written and screened by high-performing physician authors that are updated on a regular basis to ensure our SmartBanks stay up-to-date with exam blueprint changes. Below are two free emergency medicine sample questions, with complete answers. One is from our ABEM ITE question bank and the second is from our ABEM Qualifying q-bank.
Free ABEM ITE Sample Question
A 67-year-old man presents to the emergency department complaining of worsening dyspnea over the last several days. The patient knows that he normally takes medications and is unaware of his past medical history. On exam he has increased jugular venous distention. His temperature is 37°C (98.6°F), pulse is 95/min, respirations are 22/min, oxygen saturation is 82%, and blood pressure is 130/87 mmHg. Which of the following significantly increases the likelihood of the most likely diagnosis?
- A. B-type natriuretic peptide level of 267 pg/mL
- B. No response to bronchodilator therapy
- C. S3 heart sound
- D. S4 heart sound
Answer and Explanations
Did you get it right? The correct answer is C.
Although often difficult to hear, an S3 heart sound can be heard around 25% of the time in patients with heart failure. When a patient does have an S3, the likelihood for heart failure is significantly increased. The S3 heart sound comes after the normal S1 and S2 where the S4 sound comes just before the S1. Jugular venous distention can be found in around half of heart failure patients. In patients with acute heart failure but no known history of the disease, jugular venous distention, pedal edema, and cardiomegaly may be absent.
Incorrect Answer Explanations
Answer A: B-type natriuretic peptide (BNP) levels from 100-500 pg/mL have an indeterminate association to heart failure with a likelihood ratio of only 1.8. Levels over 500 pg/mL are highly associated with heart failure, with a likelihood ratio of 8.1.
Answer B: Lack of response to bronchodilator therapy does not help increase the likelihood of heart failure. Edema caused by heart failure can cause wheezing or rhonchi similar to asthma.
Answer D: An S4 heart sound is more associated with aortic stenosis and hypertrophic cardiomyopathy.
Bottom Line
Clinical signs and symptoms of heart failure include an S3 gallop, pedal edema, shortness of breath, and orthopnea. Diagnostic clues include cardiomegaly with increased pulmonary vascular congestion on chest x-ray and a BNP greater than 500 pg/mL.
For more information, see:
Rosen 9th edition, Chapter 71 Heart Failure
Get More Free ABEM ITE Practice Questions
Free TrialFree ABEM Qualifying Sample Question
A 23-year-old gravida 2, para 1 woman at 10-weeks gestation presents to the emergency department with complaints of sudden onset moderate and intermittent LLQ abdominal pain starting prior to arrival. The patient has no history of pelvic inflammatory disease or ectopic pregnancy. The patient notes no difficulty with eating or drinking and denies any surgical history. Ultrasound reveals normal adnexa and a normal intrauterine gestation. B-hCG testing reveals a quantitative level of 1231 U/mL. The patient appears very uncomfortable on exam and exhibits tenderness with guarding to palpation in the left lower quadrant. Which of the following should be performed next given the most likely diagnosis?
- A. Consult with OB/GYN for possible surgical intervention
- B. Provide analgesia and have the patient follow-up with OB/GYN within the next month
- C. Perform CT scan of the abdomen and pelvis for further evaluation
- D. Perform MRI of the abdomen and pelvis for further evaluation
Answer and Explanations
The correct answer is: A
The correct answer is to Consult with OB/GYN for possible surgical intervention.
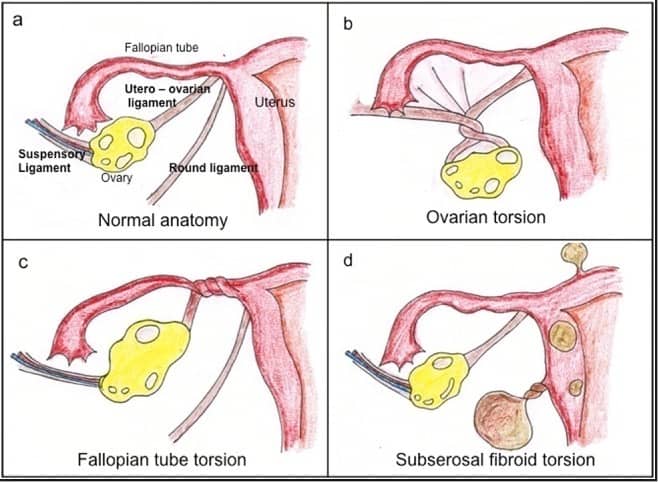
Approximately 1/5 of ovarian torsion cases occur during pregnancy, with the majority being within the first trimester. The increase in the size of the ovaries secondary to increased levels of estrogen is thought to play a role as is increased ligamentous laxity. The diagnosis is a true surgical emergency and is often missed secondary to a vague presentation of moderate, intermittent lower quadrant abdominal pain.
Ultrasound is largely non-specific, and up to 60% of patients with ovarian torsion have a normal ultrasound. Arterial flow is largely normal in these studies likely because arterial insufficiency is a late finding. Some studies have shown increased sensitivity for torsion by assessing venous flow, however despite advances in ultrasound technology most of these patients have normal ultrasound findings.
If clinically concerned, consultation with OB/GYN for possible surgical management is reasonable given the severity of this diagnosis. If the ovary becomes persistently torsed, rapid ischemia and ovary death can ensue. Therefore, these patients should ideally be evaluated by specialty care before discharge if available.
Incorrect Answer Explanations
Answer B: Although discharge is not completely out of the question, this would not be the best answer. Consultation while in the emergency department with OB/GYN would be the best next step followed by short-term follow-up with OB/GYN, ideally with an appointment made from the emergency department within the next 1-2 days. A month follow-up may be too long.
Answer C: CT scan should obviously be avoided in pregnancy, however if OB wishes to have this study performed the risks and benefits should be explained to the patient before a decision is made. This is not the best next step as the question asks.
Answer D: MRI is a possible imaging modality, however consultation with OB/GYN should be performed first.
Bottom Line
Patients suspicious for ovarian torsion should be seen by specialty care as soon as possible.
TrueLearn Insight
“Next step” questions are notoriously difficult secondary to the “shotgun” nature of a real emergency department.
For more information, see: Tintinalli 8th edition, Chapter 99 Comorbid Disorders in Pregnancy

