Leveraging Dual Coding Theory in Teaching to Maximize Learning

Healthcare educators face the complex challenge of helping learners make sense of large volumes of clinically relevant information quickly and accurately. From foundational science to clinical decision-making, the cognitive demands are high, and the time to teach is limited.
Even when content is well-structured and instruction is clear, many learners still struggle to retain and apply what they’ve learned. The issue often isn’t comprehension—it’s overload. Traditional approaches that rely heavily on verbal instruction or text-based materials can overwhelm working memory and limit the brain’s ability to store and retrieve information effectively.
This is where cognitive science offers actionable insight.
Dual Coding Theory (DCT), a well-established model in cognitive psychology, explains how learning improves when verbal and visual information are combined. Rather than relying on passive instruction or tailoring content to assumed learning styles, DCT helps educators create more effective, brain-aligned learning experiences. It’s especially valuable in environments where comprehension and retention directly impact real-world performance—like healthcare education.1
In this blog, we’ll explore:
Understanding why Dual Coding Theory matters is only the first step. To apply it effectively in teaching, it’s important to understand the cognitive science behind how it works.
What Dual Coding Theory Is
At its core, Dual Coding Theory is the idea that the brain organizes information through two distinct but connected systems: a verbal system, which processes language, and a non-verbal system, which handles visual and spatial information. Each system encodes its own kind of mental representation—or cognitive structure—in response to stimuli. For example, hearing the word “cello” activates a linguistic code, while seeing a diagram of the instrument engages the visual system.
More powerful learning occurs when these two systems communicate. Paivio referred to these cross-system linkages as referential connections—mental pathways that allow the brain to associate words with corresponding imagery.2 The richer and more interconnected these pathways, the easier it becomes for learners to recall information, differentiate concepts, and integrate new material with what they already know.
Other learning science frameworks further reinforce this principle. Cognitive Load Theory suggests that presenting material through multiple channels—such as combining diagrams with spoken explanations—lightens the burden on working memory, freeing up capacity for deeper understanding.3 Likewise, Mayer’s Multimedia Learning Theory emphasizes that learners achieve stronger outcomes when instruction pairs words with visuals, compared to using either modality in isolation.4

Cognitive overload is one of the biggest barriers to effective learning in healthcare education. Understanding how learners process, store, and apply new information can help educators design more efficient, outcomes-driven instruction.
Explore practical strategies to reduce extraneous load, improve knowledge retention, and structure content for better clinical reasoning.
Cognitive overload is one of the biggest barriers to effective learning in healthcare education. Understanding how learners process, store, and apply new information can help educators design more efficient, outcomes-driven instruction.
Explore practical strategies to reduce extraneous load, improve knowledge retention, and structure content for better clinical reasoning.
Dual Coding Theory isn’t about catering to learning styles—it’s about aligning instruction with how the brain is built to learn.
Understanding the theory is one thing. Seeing how it improves real learning experiences is what makes it practical. In healthcare education, where cognitive load is high and performance matters, Dual Coding Theory offers a clear framework for helping learners build stronger, more retrievable knowledge.
Real-World Examples of Dual Coding Theory in Healthcare Education
Instructional strategies that integrate verbal explanations with visuals align directly with the principles of Dual Coding Theory. When applied intentionally, they improve retention, reduce mental strain, and strengthen learners’ ability to apply concepts in clinical environments.
Anatomy and Physiology Instruction
In foundational and advanced settings, educators often combine spoken or written explanations with anatomical diagrams, 3D models, or cadaver dissections. This pairing helps learners encode complex spatial relationships and physiological functions more effectively by engaging both the verbal and visual systems.
Multimedia for Clinical Skill Development
Video-based demonstrations of procedures like intubation or ultrasound imaging, accompanied by verbal narration, help learners link steps with clinical reasoning. This combination of modalities improves learners’ ability to mentally rehearse and apply skills, especially when followed by simulation or hands-on practice.
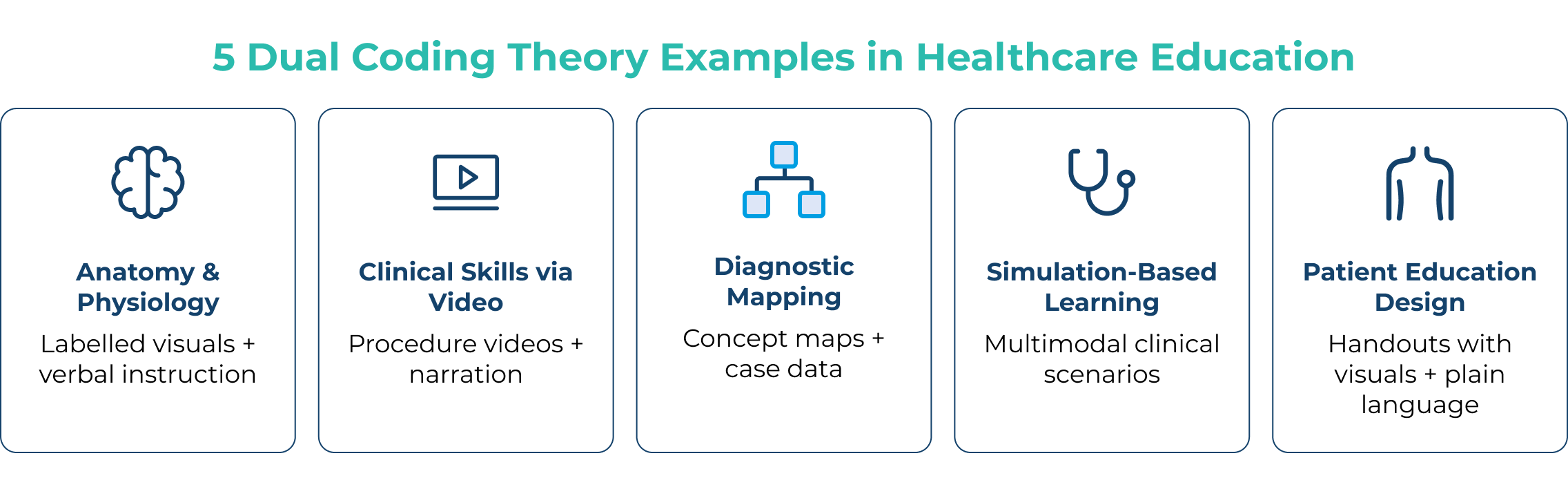
Visual Tools for Diagnostic Reasoning
Concept maps, clinical flowcharts, and decision trees provide visual frameworks that complement verbal or case-based instruction. These tools help learners organize clinical information and build the pattern recognition needed for accurate diagnosis.
Simulation-Based Learning
Simulation environments are inherently multimodal. Learners receive verbal instructions, observe physical signs, interpret visual cues, and respond with hands-on interaction. This layered experience supports deeper encoding and mirrors the cognitive demands of clinical decision-making.
Designing Patient Education Materials
When learners create educational handouts for patients, they apply the core principles of Dual Coding Theory. Explaining medical conditions using clear language alongside visual diagrams not only supports patient understanding but also reinforces the importance of delivering content in ways that align with how people learn best.
These examples demonstrate that dual coding theory in education is not limited to traditional classroom instruction. In healthcare education, it plays an active role in helping learners connect, retain, and apply complex information with confidence.
How to Bring Dual Coding Theory into Healthcare Education
While Dual Coding Theory often shows up in everyday instruction, its real impact comes from being applied intentionally. This means thinking critically about how learners engage with information—not just what we teach, but how it’s presented.
This approach aligns with the principles of multimodal learning, which emphasizes delivering content through multiple sensory channels to enhance cognitive processing and retention. Rather than relying on outdated notions of “learning styles,” this strategy is grounded in how the brain actually learns—by integrating and reinforcing information across verbal and visual systems.
Healthcare educators don’t need to overhaul their curriculum to apply Dual Coding Theory effectively. Small, strategic changes in content design and delivery can create more durable, transferable knowledge.
Use visuals with intention
Incorporate diagrams, flowcharts, and clinical imagery that directly support your instruction.5 Visuals should reinforce, not distract from, the verbal explanation—whether you’re illustrating a pathophysiological process or outlining steps in a procedure.
Apply dual coding across different settings
In the classroom, pair spoken lectures with annotated slides or animations. In clinical teaching, use visual prompts—like diagnostic images or quick-reference cards—alongside verbal guidance to reinforce key takeaways.
Encourage learners to generate their own visuals
Ask learners to sketch disease mechanisms, draw out case progressions, or create mind maps that connect clinical signs to underlying causes.6 This kind of active translation from verbal to visual strengthens encoding and long-term recall.
Incorporate audiovisual mnemonics
Mnemonics that combine visuals, sounds, and rhythm—such as animated videos or image-based memory cues—can help learners quickly encode and retrieve complex information.7 These tools activate both the verbal and non-verbal systems, making them especially effective for supporting long-term recall in content-heavy areas.
Leverage technology to support dual coding
Use tools that combine visual and verbal elements, such as multimedia simulations, adaptive quizzes with image-based prompts, or digital whiteboards that enable concept mapping. These platforms model the principles of dual coding at scale.
Design assessments with both inputs
Integrate visual cues—such as imaging, graphs, or clinical photos—into written assessments. Asking learners to interpret both types of information mirrors real diagnostic scenarios and reinforces knowledge retrieval through multiple pathways.8
By aligning instruction with how the brain processes information, healthcare educators can help learners absorb, retain, and apply knowledge with greater clarity and confidence.
Dual Coding Theory provides more than just insight into how learning works—it offers a practical approach to designing instruction that supports deeper understanding and long-term retention. From structuring content to guiding clinical reasoning, intentionally pairing verbal and visual information empowers learners to make stronger connections, think more critically, and perform more confidently—both in training and in practice.
Want to know how you can bring the principles of Dual Coding Theory into your curriculum?
Explore how TrueLearn’s precision learning tool integrates cognitive science, adaptive learning, and audiovisual mnemonics to help your program improve retention, build clinical decision-making skills, and drive stronger outcomes across every stage of healthcare training.
References & Footnotes
1 Clark JM, Paivio A. Dual coding theory and education. Educ Psychol Rev. 1991;3(3):149-210. doi:10.1007/bf01320076
2 Paivio A. Mind and Its Evolution: A Dual Coding Theoretical Approach. Psychology Press; 2014. doi:10.4324/9781315785233
3 Sweller J. Cognitive Load Theory. In: Psychology of Learning and Motivation. Elsevier; 2011:37-76.
4 Mayer RE, ed. Cambridge Handbooks in Psychology: The Cambridge Handbook of Multimedia Learning. 2nd ed. Cambridge University Press; 2014.
5 Challa KT, Sayed A, Acharya Y. Modern techniques of teaching and learning in medical education: a descriptive literature review. MedEdPublish. 2021;10(1):18. doi:10.15694/mep.2021.000018.1
6 Daley BJ, Durning SJ, Torre DM. Using concept maps to create meaningful learning in medical education. MedEdPublish. 2016;5(1):19. doi:10.15694/mep.2016.000019
7 Arora B, Giri JN. Dual coding theory and its application in healthcare facility. Int J Health Sci (IJHS). Published online 2022:5021-5025. doi:10.53730/ijhs.v6ns2.6261
8 Donkin R, Yule H, Fyfe T. Online case-based learning in medical education: a scoping review. BMC Med Educ. 2023;23(1):564. doi:10.1186/s12909-023-04520-w
![Strategies To Encourage Independent Strategic Learning [Educator Webinar]](https://truelearn.com/wp-content/uploads/2021/06/Educator-Webinar-Strategies-To-Encourage-Independent-Strategic-Learning.png)